Paruresis (Shy Bladder Syndrome)

For a very long time, Alex didn’t think of it as a problem, but now, looking back, he realises the signs have been there for a while.
Alex could urinate at home without any effort. At work, he would usually wait until the bathroom was empty. If there was another person there, it took Alex slightly longer to initiate peeing as he felt a bit self-conscious, but he didn’t think much of it.
One day, Alex went to a crowded restroom at a restaurant over his lunch break. There were people waiting to use the urinals. Alex suddenly felt rushed, watched, and under pressure. He tried to pee quickly, but was unable to produce any stream. He left the restroom feeling humiliated and sensing what seemed like mocking and disapproving stares.
After that, he started paying attention, doing whatever he could to avoid being in this position again.
He began timing when he drank water, which gradually led to more and more restrictions of his fluid intake. Choosing certain bathrooms over others. Peeing “just in case” whenever he had access to a “safe” restroom. Switching from urinals to stalls because they felt safer. He also discovered that it was easier to pee when sitting on a toilet than when standing while using a urinal. But still, if someone walked in, his body locked up. Alex tried to relax and to wait, but the more he tried, the more difficult it was to produce the stream. He would sometimes leave the bathroom, walk around for a few minutes, and come back to try again. Over time, he became worried that others might notice this pattern, and stopped coming back altogether. This led to even more pressure to urinate on the first attempt and even greater difficulty producing a stream.
Over time, the problem spread. Bathrooms that used to be fine stopped working. Even stalls felt impossible if there was any chance that someone could be waiting. Airports, planes, and road trips became a nightmare and he would decline travel whenever possible. Alex consumed less and less fluid during the day, stopped drinking any caffeinated beverages, and avoided situations where bathrooms felt unpredictable. He held urine for increasingly prolonged periods, ignoring physical discomfort.
Now the anxiety started long before he even entered the restroom. Even the thought of a public bathroom became a trigger, often hours before he would actually need to go. He made sure to mentally map “safe bathrooms” in advance to be prepared and would detour significantly out of his way just to reach one. He sometimes used a single-occupancy, lockable bathroom in a hotel 20 minutes walking distance from his work (which was still tricky as somebody could potentially be lining up outside the door and Alex had no way of knowing that).
The bathroom in Maya’s university apartment that she shared with her roommates was just outside the living room. Maya, a first-year university student, had no difficulty using it to pee when she was alone in the apartment or when her roommates were watching a movie. The problems started when it was quiet in the apartment and her roommates were nearby. Maya would try to use the bathroom to pee but felt pressured, as she felt her roommates might be wondering why it was taking her so long. The more pressured she felt, the more difficult it was to produce the stream.
This became even more challenging in the mornings, as Maya knew that her roommates would be waiting to use the bathroom. She peed while taking the shower with no problem. But on the mornings when she didn’t have time to shower, she would still have the water running, and it really helped.
Public restrooms at university were harder. She couldn’t have water run there, and she could not handle the lines and the thin walls between the stalls.
Maya started adjusting. She avoided drinking any fluids before going to school and stopped carrying her water bottle. Peed “just in case,” when she had an opportunity, even when she didn’t really need to. She learned she could sometimes force it by straining or squeezing, even though it felt uncomfortable. She learned which positions were more likely to lead to successful urination and became over-reliant on positions and breathing patterns. When it worked, she told herself she’d found a solution, but then, when it didn’t, she felt defeated.
When she heard people lining up outside talking, she wondered if they were discussing her. When there was silence outside, she interpreted it as scrutiny.
To escape after fruitless attempts to urinate, Maya would wait for a hand dryer to activate or some other external noise, flush the toilet, and exit pretending to be on her phone to avoid other women’s gazes. She wondered if people waiting in line knew that something was wrong with her and were secretly judging her. She often noticed the girls in the line giving each other a look and a smile, and she was sure they knew. Shame and humiliation stayed with her for a long time. Sometimes the feeling lingered for hours or even the rest of the day.
Maya was also dreading the next uni class, knowing that her bladder was full. This made her fluid restriction even more severe.
Maya left events early. Avoided trips. She panicked before long drives and began structuring outings around where and when she might be able to pee. She said no to things she actually wanted to do. Bathrooms stopped being neutral places and became obstacles she had to manage. Sometimes alcohol helped her pee, but other times it made things worse.
Maya started wondering if something was physically wrong. She finally went to see a doctor, but her UTI test came back negative, and the doctor told her to just relax.
What is Paruresis (Shy Bladder Syndrome)
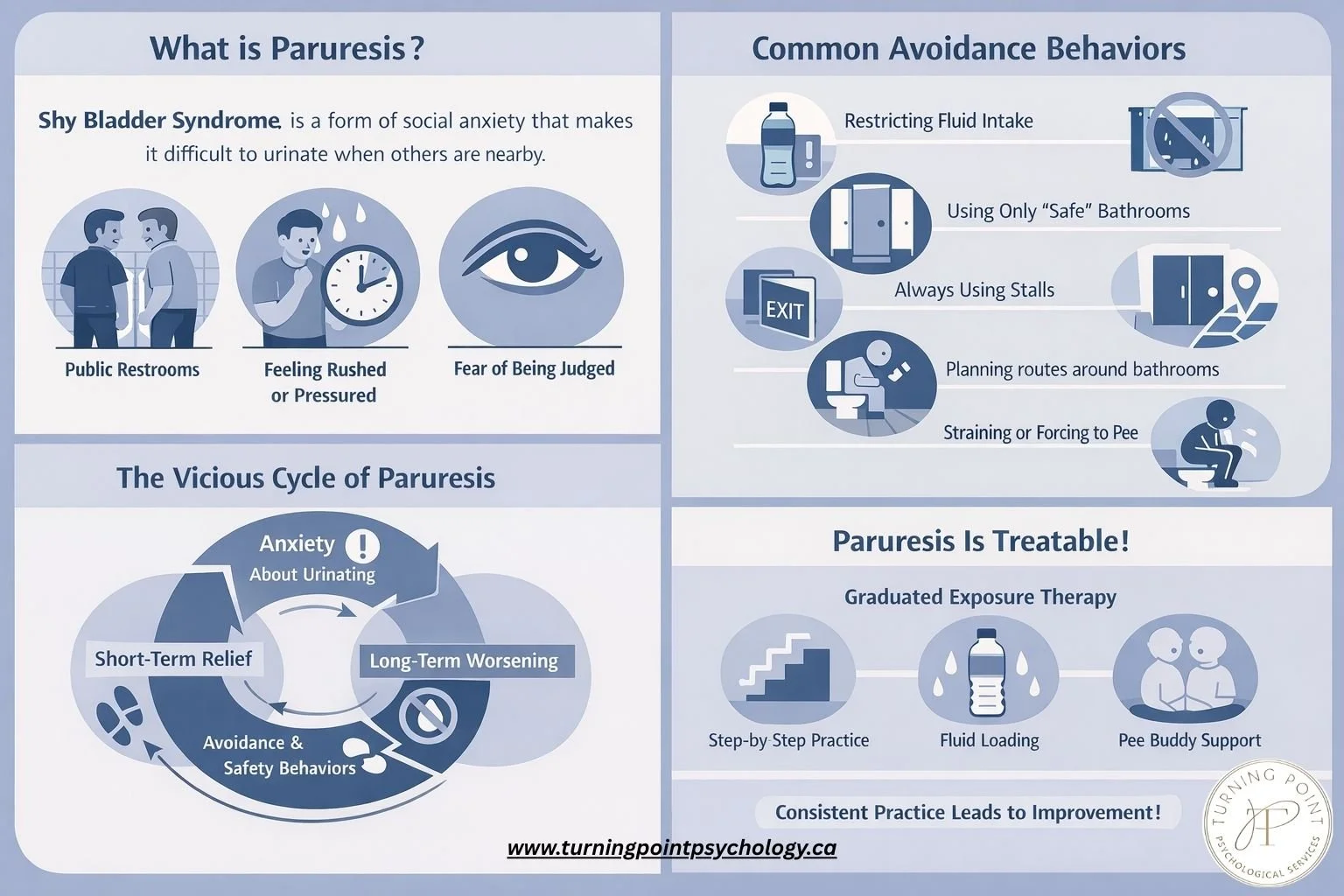
Paruresis (shy bladder syndrome) is a form of social anxiety characterized by difficulty urinating when other people are nearby or could be nearby. A person with paruresis can urinate without any difficulty when alone at home, but may struggle in public restrooms and in situations where somebody could hear, see, or be waiting.
Paruresis can look different from person to person. For some, it shows up as a delay or hesitation before the stream starts. For others, it can feel like a complete shutdown. Some people struggle only in certain places, while others find the difficulty spreads over time to more and more situations.
A common misunderstanding is that paruresis is a fear of urinating in front of others. But in reality, the core fear is usually about not being able to urinate when others are nearby.
Main triggers of paruresis include public restrooms where other people may be present, feeling rushed, anxiety about being unable to produce a stream or producing a very weak stream, and worry about being judged for how long it takes. Factors such as silence, thin walls between stalls, or a lineup outside the washroom may further increase anxiety.
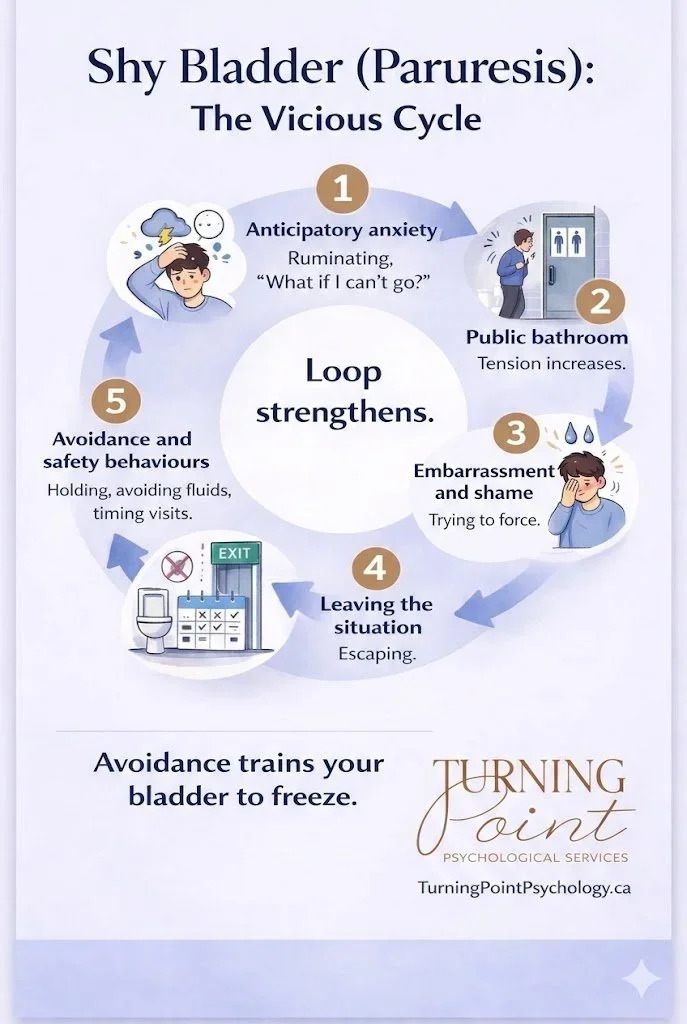
Paruresis usually worsens with time. In an effort to cope, people start adjusting what they drink, where they go, and how they use the bathroom. These strategies can reduce anxiety in the moment, but over time they reinforce the problem and allow it to spread to more and more situations.
How to Rule Out a Medical Cause of Paruresis
There are some tests that may be indicated to rule out medical conditions such as a urinary tract infection (UTI), cystitis, or an enlarged prostate.
But, if you have no difficulty urinating when you are alone at home, while struggling when other people may be nearby, it’s probably paruresis.
Common safety and avoidance behaviours of people with paruresis include:
· Restricting fluid intake (which makes urination even harder)
· Urinating “just in case” whenever a familiar or “safe” bathroom is available
· Trying to identify and use only “safer” bathrooms
· Avoiding urinals and relying only on stalls, or only specific stalls
· Avoiding travel, long meetings, events, or social plans
· Leaving events early
· Declining invitations that involve travel, lines, or time pressure
· Planning routes and days around available bathrooms rather than activities
· Running water, flushing early, or waiting for hand dryers to create cover noise
· Using specific body positions or breathing patterns believed to make it easier
· Straining, squeezing, or forcing the stream
· Holding urine for long periods
· Using alcohol
Although these strategies feel necessary, they gradually narrow the range of situations in which urination feels possible, making paruresis generalize to additional situations.
Paruresis Treatment
The most effective treatment for paruresis is graduated exposure therapy - a structured repeated practice in increasingly challenging bathroom situations. In our clinic, we find that combining graduated exposure with ACT (Acceptance and Commitment Therapy) makes the treatment even more effective.
Treatment includes creating a clear plan – a hierarchy - to gradually attempt to urinate in different situations starting with those that feel the least challenging and progressively increasing difficulty over time. Treatment also includes fluid loading before exposure practice. This is done to increase the urge to urinate, making initiating a stream easier.
Whenever possible, it can also be helpful to involve a pee buddy — a trusted person with whom you feel comfortable. A pee buddy may stand nearby, wait outside the restroom or stall, enter the restroom together, or help recreate real-world conditions in a gradual way. For many people, practicing exposures with a trusted person can make the process feel more manageable and reduce avoidance early in treatment.
Can Paruresis Be Cured?
Yes. With structured exposure-based treatment, most people experience significant improvement, and many are able to urinate comfortably in situations that once felt impossible. The key is consistent, graduated practice rather than trying to force relaxation or eliminate anxiety first.
A typical paruresis treatment plan may include:
· Assessment of how paruresis developed, how it changed over time, and what currently triggers it (both internal and external triggers).
· Identifying current overt and covert safety and avoidance behaviours.
· Psychoeducation about paruresis, including how safety and avoidance behaviours maintain it, and how fluid loading is used in treatment.
· Learning ACT-based strategies to support motivation, willingness, and persistence during exposure practice.
· Creating a personalised exposure hierarchy.
· Identifying a reliable backup restroom for early exposure work.
· When possible, recruiting a pee buddy – a trusted person who can support exposure practice.
· Fluid loading prior to exposure.
· Practicing exposure tasks between sessions, reviewing progress, and adjusting strategies as needed.
Why Paruresis Is Often Missed or Misunderstood
Paruresis is very common, but is underdiagnosed because:
· People are embarrassed to talk about it
· Many assume it’s a quirky habit or a personal flaw and don’t realize it’s a known and treatable psychological condition
· Even if a person seeks help, health professionals may not recognise paruresis. People are often referred for medical tests that come back normal, without further explanation
Even when a mental health professional recognizes that this is an anxiety disorder, one key misunderstanding often remains: assuming that the person is fearful of urinating in the presence of others. The treatment (usually Cognitive Behavioural Therapy (CBT)) based on this assumption may include exposure exercises that miss the real fear, leading to little improvement. This leads to a lot of confusion and despair.
The problem is subtle but important: in most cases, the fear is not about urinating in the presence of others. It’s about NOT being able to urinate when others might be nearby. This nuance changes how exposure is planned and what the person is actually practicing. For this reason, it is important to work with a therapist who has specific knowledge and experience treating paruresis rather than treating it as generic social anxiety.
If parts of this felt uncomfortably recognisable, there’s nothing unusual or “wrong” about you. Paruresis follows a very consistent pattern, even though it can feel deeply personal and isolating when you’re living with it.
What keeps shy bladder going is not the bladder itself, but the way anxiety, pressure, and well-intended coping strategies interact over time.
Many people feel a sense of relief when they finally recognise their own experience in this pattern. Paruresis can feel deeply personal and isolating, but it is surprisingly consistent in how it develops and how it responds to treatment.
The encouraging part is that this also makes it very treatable. People often see meaningful improvement once the pattern is properly understood and addressed — even if they’ve been struggling for years.
For people who want support, working with a therapist who has specific experience treating anxiety disorders and paruresis in particular, can make the process more effective and straightforward.
Where to Start If This Sounds Like You
Shy bladder is maintained by avoidance and control. The way out is gradual, repeated practice in the situations you’ve been avoiding. Here is where to start.
14 Practical Strategies to Start Overcoming Paruresis
1. Rule out medical causes.
If you cannot urinate even when alone at home, or you have pain, weak stream, frequent small volumes, or other physical symptoms, get checked medically.
If you can urinate normally at home when alone but struggle mainly when others are nearby (or might be nearby), you’re likely dealing with paruresis.
2. Stop trying to control when you need to go.
It is very common for people with paruresis to try to restrict fluids - sometimes very aggressively. Fluid restriction feels protective. But drinking less, “going just in case,” urinating on a schedule, or emptying your bladder repeatedly before leaving home just keeps the paruresis vicious cycle going. As with all anxiety disorders, control is the problem, not the solution.
Start reversing this:
Drink normally.
Stop restricting fluids before outings.
Stop “pre-emptive” urinating unless you truly need to go.
Let your bladder fill.
A full bladder increases your physiological odds of success. Trying to urinate with low urgency makes misfires (not being able to pee) more likely and reinforces the shy bladder.
3. Only practice when you genuinely need to go.
Trying to urinate when your bladder is only half-full sets you up for unnecessary struggle.
Wait until your urgency is reasonably high before going.
Let your body work with you, not against you.
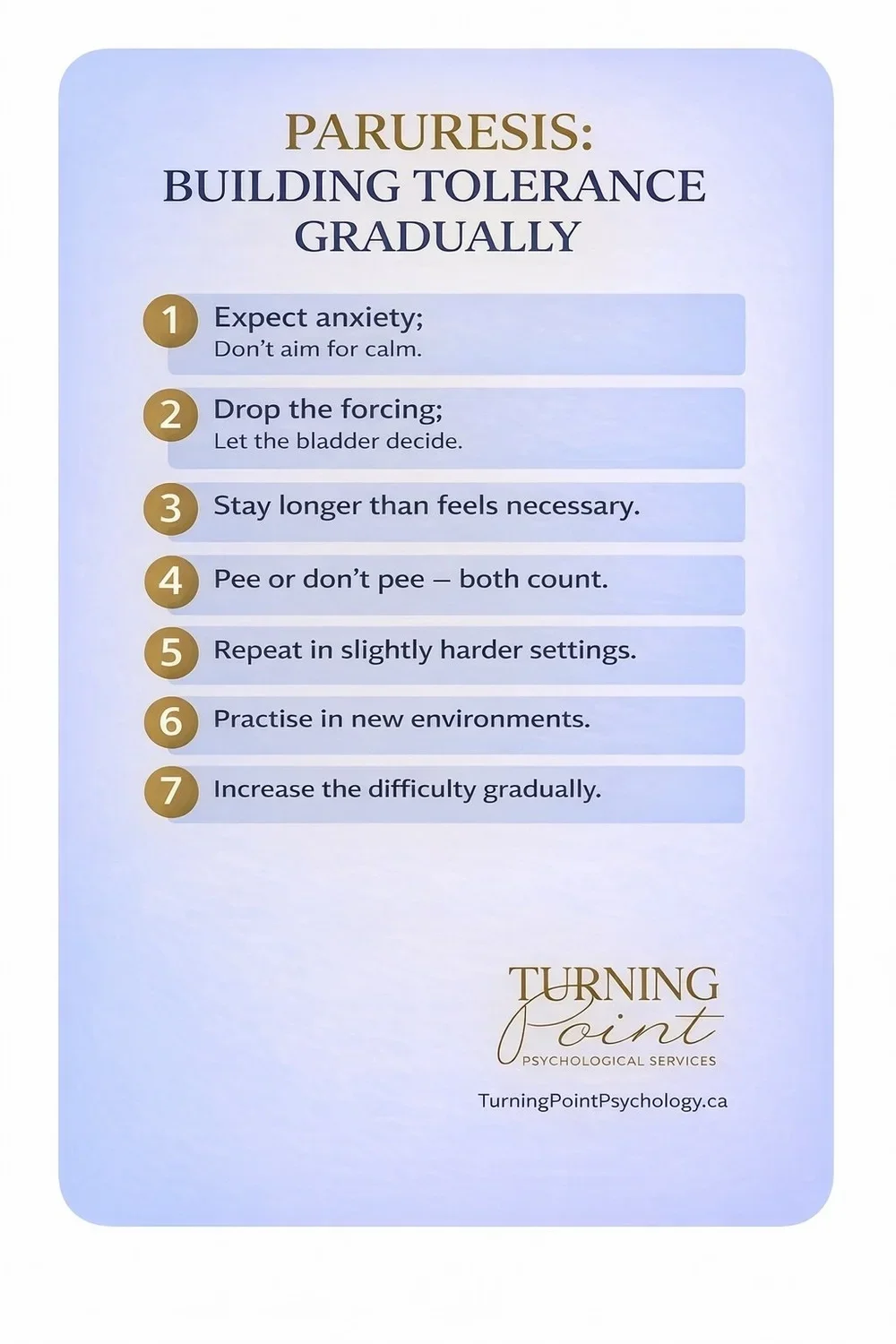
4. Drop the language of “success” and “failure.”
You either urinate or not. Both are part of practice. The goal of the treatment is not to win a medal for a pee performance, but to show up and continue practicing. If you pee in a public washroom - that’s amazing. And if you don’t - that’s just as much of a win as you learn that it wasn’t the end of the world and you can continue practicing next time.
5. Build a gradual exposure ladder.
Start with situations that are slightly uncomfortable but doable, then move up gradually.
Examples:
Home bathroom with someone in the house
Door unlocked
Someone standing outside
Quiet public washroom
One person present
Busier washroom
Urinal instead of stall for guys
Peak traffic settings (workplace, airport, game, concert)
6. Practice frequently and intentionally.
Practice all the time. Ideally, several times per day.
Stay in the situation long enough to let your nervous system settle.
Repeat attempts instead of leaving immediately after a misfire.
Track attempts and contexts to increase awareness of subtle avoidance.
7. Stop buffering the experience.
Common safety behaviors include:
Running the tap
Flushing repeatedly
Using background noise to mask silence
Choosing only isolated stalls
Waiting until bathrooms are empty
Using alcohol to “loosen up”
Avoiding urinals entirely
Leaving the moment you sense someone nearby
These behaviors temporarily reduce anxiety, but maintain it in the long run. Notice them and gradually remove them.
8. Intentionally increase “pressure” in controlled ways.
Once basic exposures improve:
Go during busier times.
Choose random stalls.
Use different washrooms.
Go right before meetings.
Arrive slightly late and tolerate the discomfort.
Practice when someone passes behind you.
Practice with mild time pressure.
9. Expect inconsistency.
You may go easily one day and struggle the next. This is normal. Progress in paruresis, just like with other anxiety disorders is rarely linear. Do not interpret fluctuation as regression. Just continue practicing.
10. Lean into discomfort instead of negotiating with it.
The paradox of paruresis is that the harder you try to urinate, the harder it becomes.
Instead of forcing it, allow anxiety to be present. Let the “what if I can’t?” thoughts sit there. Resist the urge to escape and stay in the restroom without rushing out. That way, you are retraining your brain that bathrooms are not danger zones.
11. Reduce outcome focus.
When you go into the restroom thinking, “This better work,” you’re increasing performance pressure. Instead, shift to: “I’m practicing being here.” Concentrate on the process, not the outcome. Outcome follows process.
12. Involve someone you trust to be your pee buddy if possible.
Practicing with a partner — therapist, friend, or trusted person — can accelerate progress.
13. Normalize it.
Paruresis is far more common than people think. Many high-functioning, confident individuals experience it. It is just a learned fear pattern that can be unlearned.
14. Commit to daily life, not symptom elimination.
Drink normally.
Travel.
Attend meetings.
Go to concerts.
Use the washroom when needed.
The most common mistake that we see in patients with any kind of anxiety, including paruresis, is that they wait for anxiety to subside before doing the things they want to be doing. But the goal is not to eliminate anxiety first. It’s the other way around, that is, to live and let anxiety recalibrate in the background.
If progress stalls or anxiety escalates significantly, working with a therapist who understands exposure-based treatment can make a meaningful difference.
To summarise:
Paruresis is highly treatable.
Avoidance makes it grow.
Practice makes it shrink.
If you’re tired of planning your life around bathrooms, you don’t have to keep doing this alone. At Turning Point Psychological Services, we treat paruresis using exposure-based approaches tailored to each client. Reach out to get started.
In Short:
Paruresis is a learned anxiety response, not a physical malfunction.
Avoidance and fluid restriction maintain the cycle.
Graduated exposure retrains the nervous system.
Inconsistency during recovery is normal.
With structured practice, it is highly treatable.
Frequently Asked Questions About Paruresis
Is paruresis the same as shy bladder syndrome?
Yes. Paruresis and shy bladder syndrome are two names for the same condition - difficulty urinating when others are nearby due to anxiety. Some people also call it bashful bladder or pee anxiety.
Is paruresis a medical problem or a psychological one?
Paruresis is not caused by a bladder disease or physical obstruction. It is a form of social anxiety that interferes with urination in specific situations, despite normal bladder function.
Why can I urinate at home but not in public bathrooms?
This pattern is typical of paruresis. The difficulty is triggered by pressure, awareness of others, or the possibility of being heard or observed - not by a problem with the bladder itself.
Does avoiding fluids or planning bathrooms actually help?
Avoiding fluids or carefully planning bathrooms may reduce anxiety temporarily. However, these strategies reinforce the belief that urination is only possible under specific conditions, which strengthens paruresis over time.
Does paruresis get worse over time?
It often does. As avoidance and safety behaviours increase, the difficulty can spread to more situations and begin earlier — sometimes even before entering a restroom.
What is the most effective treatment for paruresis?
Graduated exposure therapy is considered the most effective treatment for paruresis. Many people benefit from combining exposure with Acceptance and Commitment Therapy (ACT), which helps build willingness and reduce avoidance.
Do I need to know what caused my paruresis to get better?
No. Many people improve without identifying a single cause. Treatment focuses on changing the current pattern of avoidance and anxiety rather than analysing a past event.
Can paruresis be cured?
Yes. With structured exposure-based treatment, most people experience significant improvement, and many regain the ability to urinate comfortably in situations that once felt impossible. Consistent, graduated practice is the key to retraining the nervous system.
Can paruresis improve even after many years?
it can. Even long-standing paruresis can improve once the pattern is clearly understood and addressed systematically. People are often surprised by how much change is possible.

Anna Prudovski is a Psychologist and the Clinical Director of Turning Point Psychological Services. She has a special interest in treating anxiety disorders and OCD, as well as working with parents.
Anna lives with her husband and children in Vaughan, Ontario. When she is not treating patients, supervising clinicians, teaching CBT, and attending professional workshops, Anna enjoys practicing yoga, going on hikes with her family, traveling, studying Ayurveda, and spending time with friends. Her favorite pastime is reading.










-
Anxiety
- Dec 28, 2025 Paruresis (Shy Bladder Syndrome)
- Jul 5, 2020 Anxiety and Related Disorders
- Jun 2, 2020 Panic Disorder
- Jul 7, 2019 Social Anxiety Disorder: Facts, Symptoms, Treatment, and Tips for Managing It.
- Jun 6, 2019 10 Popular Therapy Strategies that Don’t Work for Bad Anxiety or OCD
- Mar 6, 2019 10 Tips for Dealing with Anxiety
- Feb 7, 2019 Don’t Feed the Dinosaurs or How to Face Your Anxiety
- Jan 22, 2019 Meet Anxiety. Anxiety: Part 1/7
- Dec 24, 2018 Why does Anxiety Interfere with My Life So Much? Anxiety: Part 2/7
- Dec 17, 2017 Anatomy and Physiology of Anxiety. Anxiety: Part 3/7
- Dec 3, 2017 Dealing with Anxiety Components One by One. Anxiety: Part 4/7
- Nov 12, 2017 The Discovery of Oz the Terrible. Anxiety: Part 5/7
- Oct 8, 2017 Meet Your New Best Friend: Uncertainty. Anxiety: Part 6/7
- Sep 10, 2017 Some More Strategies to Help You Deal With Anxiety and Worry. Anxiety: Part 7/7
-
OCD & Co
- Nov 23, 2021 ACT for OCD: Why Fighting Intrusive Thoughts Makes OCD Worse
- Sep 13, 2021 Relationship OCD (ROCD) and Its Treatment
- Jul 12, 2021 Existential OCD
- Jun 8, 2021 Real Event OCD: Why You Can’t Stop Thinking About Past Mistakes
- Apr 17, 2021 Signs That You or Someone You Know May Have OCD and Not Realize It
- Dec 2, 2020 Don’t Argue With a Brain Glitch. (10 Do's and 5 Don'ts for Parents of Kids with OCD)
- Sep 25, 2020 Do I have OCD? 8 Surprising OCD Myths
- Aug 15, 2020 9 Surprising Things We Don’t Do When Treating OCD at Our Clinic
- May 21, 2020 Illness Anxiety and How to Overcome It
- Feb 21, 2020 OCD and Online Romance Scam
- Jun 6, 2019 10 Popular Therapy Strategies that Don’t Work for Bad Anxiety or OCD
- Nov 17, 2018 Is it Possible to Be “a Little OCD?”
- Oct 23, 2018 Defeating the (Seemingly) Indestructible OCD Hydra: 8 Effective Tricks to Deal with New Obsessions.
- Oct 22, 2018 OCD, is That You Again? How to Know if Your New Thought is OCD, and 6 Concrete OCD-Repelling Strategies for You to Start Practicing Right Away.
- Oct 21, 2018 Trich or treat? Are you secretly pulling your hair out? Trichotillomania and its Treatment
- Apr 26, 2017 Stepping Off the OCD Hamster Wheel. A Therapist's Recovery Journey
- Parenting
-
Psychology
- Aug 21, 2019 The Road to ‘Stuckness’ is Paved with Good Intentions
- Sep 4, 2018 Having Difficulty Making Decisions? This Subtle Shift in Your Perspective May Change the Way You Approach Decisions from Now On.
- Aug 17, 2018 A Gentleman in Moscow or How to Live Life
- Jul 1, 2018 Who Goes to Therapy? Myths Versus Reality: The Therapist’s Perspective
- May 1, 2018 Do you often ask this innocent question? Watch out – you may be at risk for depression, anxiety, and other disorders.
- Feb 3, 2018 An effective hack to instantly take the edge off a negative emotion